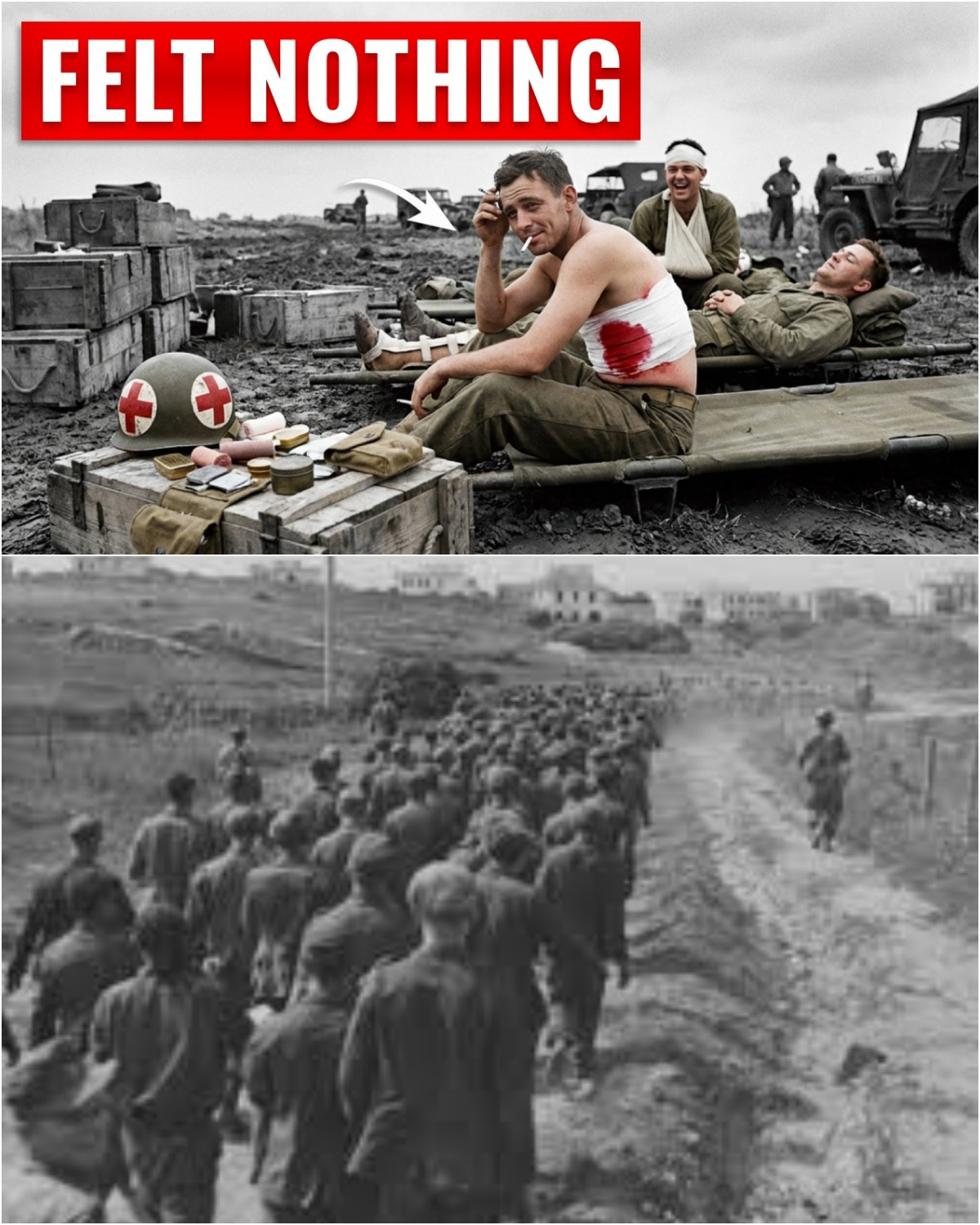
On the 16th of February 1944, at a German forward surgical station four miles south of Cesterna on the Anzio beach head in Italy, a medical officer was sorting through a line of casualties when a group of American prisoners was carried in on stretchers. The fighting around Anzio had been grinding both armies down for 3 weeks.
A German counteroffensive had launched that morning, and the surge of wounded overwhelmed every aid station within miles. Among the casualties arriving at this HopVaban plots were nine Americans captured during the fighting. Men with shrapnel wounds, compound fractures, one with a perforated abdomen. The German doctor had been treating combat wounded since the Eastern Front.
He knew what a man with a shattered femur sounded like. He knew the pitch of a scream that came with steel buried near a man’s spine. But these Americans were different. Some lay still on their stretchers, watching the German orderlys with flat, steady eyes. One was trying to light a cigarette with a hand that was missing its thumb.
A private with a hole torn through his right side, a wound large enough to see the muscle wall beneath, was sitting up and asking for water in broken Italian. They were not screaming. That would have troubled any doctor on any front, but it especially troubled a German doctor in 1944 because in more than two years of cutting and suturing German soldiers with identical injuries, he had almost never seen men absorb this kind of damage in silence.
Not without an injection from a medical officer, not without sedation administered at a hospital. And these Americans had not come from any hospital. They had come straight from the field in their own bandages, captured before any surgeon reached them. Something had gotten to them first. He just did not know what. If the story of what these American soldiers endured deserves to be heard, hit subscribe and the like button.
It takes 2 seconds and helps these histories reach people who care. About 30 m to the southeast at a Ford hospital on the same beach head, an American was looking at the same mystery from the other side. Henry Beecher was 40 years old, a Harvard trained anesthesiologist, the first person in the world to hold an endowed chair in the field of anesthesia.

He had been treating combat wounded since North Africa. And what he was observing at Anzio contradicted everything he thought he understood about how the human body processes pain. Here is what Beecher found. Pay attention to this number because it will change meaning before this story is over. He examined 215 soldiers who had sustained major wounds during the prolonged fighting at Anzio on the Venafro front and along the approaches to Casino.
These were not light injuries. Penetrating abdominal wounds where blood and intestinal contents had spilled into the body cavity. Compound fractures of the femur and tibia. Extensive soft tissue destruction from high explosive fragments. Men whose bodies had been torn open in ways that should have been unbearable. He asked each man a single question.
Is your pain bad enough that you want something for it? Three out of four said no. Not three out of four men with scratches. Three out of four soldiers with wounds that in a civilian hospital in Boston would have had every patient demanding morphine before the stretcher reached the hallway. Beecher later ran precisely that comparison.
Same type of injury, civilian surgical ward, and found the numbers nearly inverted. In Boston, the overwhelming majority wanted immediate relief. At Anzio, 75% of men with equivalent wounds said they did not need it. The question was why? Beer spent years on that question. He published a landmark paper, Pain in Men Wounded in Battle Annals of Surgery, January 1946, and proposed an answer that had nothing to do with courage or toughness.
He believed the meaning of the wound changed the experience of the pain itself. For a soldier, a serious wound meant one thing above all: survival, evacuation, home. The body was broken, but the danger was over. For a civilian, the identical injury meant the opposite, the beginning of danger. But that was only part of what was happening at Anzio.
Because Beecher was studying men who had already arrived at his hospital, men who had been found, stabilized, bandaged, and transported to the rear. What he did not examine, what no American doctor at the time thought to examine because it was so ordinary they could not even see it, was everything that happened to those soldiers between the instant the steel entered their bodies and the moment they appeared on his operating table.
That invisible window, those first minutes in the dirt, before any surgeon, before any hospital, before any ambulance, is where this story begins. Because inside that window, the United States Army had quietly built something no other army in the world possessed. It was not a weapon. It was not a tactic. It was a system so small that its central instrument fit inside a man’s palm, and so silent it made no sound at all.
It reached a wounded American soldier while he was still lying where he fell and changed what happened inside his body before any doctor was involved. Here is the part that should stop you. The Germans had morphine. They had not merely acquired it. They had created it. A German chemist named Friedri Sir Turner first isolated morphine from raw opium in 1804, 40 years before this war’s grandfathers were born.
The company that first mass-produced it, Merc, was German. The company that refined it into the derivative they marketed as heroin, Bayer, was also German. And yet, on the 16th of February, 1944, when a German medical officer stood over a row of American prisoners with shattered bones and torn abdomen, and could not explain why they were not screaming, he did not know that the answer was a half grain of morphine tartrate sealed inside a collapsible tin tube the size of a man’s little finger.
He did not know because in the entire German army, that tube did not exist. What existed instead and what it cost every German soldier who ever lay bleeding in a ditch waiting for help that the system was never built to send goes far deeper than any single drug. It begins not with morphine but with a question the German army never thought to ask.
The question the German army never thought to ask was deceptively simple. What does a wounded soldier need in the first 5 minutes after he is hit? Not the first hour, not the first day, the first 5 minutes while he is still lying where he fell with dirt in the wound and steel in the bone before any stretcher exists in his world.
What does he need right then? The American army had an answer. And in early November of 1943, weeks before the Anzio landings, during the grinding advance through Venifro in southern Italy, that answer created a problem nobody expected. Surgeons working in the forward operating tents began seeing something they could not account for.
Wounded men arrived from the field in shock, chilled through, gray-faced, all presenting the same collapsed appearance. Standard procedure, warm them, push fluids, treat for shock, prepare for surgery. Most responded normally, but some of them after receiving exactly the same warming, the same fluids with no morphine administered at the hospital suddenly developed pinpoint pupils, respiratory depression, and a pulse that was sliding toward nothing.
Classic morphine poisoning, textbook overdose. These men had not been given a single drop of morphine since entering the hospital. The morphine was already inside them when they arrived. Think about what that means. Somewhere between the spot where these soldiers were hit and the operating tent where surgeons opened them up, someone had injected them with morphine.
In many cases, more than once. The November cold had slowed their circulation so severely that the first dose never seemed to work. The wounded man kept groaning, kept shaking, and whoever was kneeling beside him in the dirt had broken the seal on a second tube, sometimes a third. When the men were finally warmed and their blood started moving again, all three doses hit the bloodstream at once.
The army had to issue warnings. Not because soldiers were being denied pain relief, but because they were getting too much of it too fast, too far forward. The instrument at the center of this was a collapsible tin tube about the length of a man’s thumb with a short hypodermic needle fixed to one end and a wire loop pin crimped to the other.
It weighed almost nothing. It fit inside a pocket, a pouch, a first aid packet. It was called a set. To use it, you needed no medical degree, no sterile syringe, no glass vial. You pulled off the transparent plastic cap, pushed the wire loop through the inner seal to puncture it, withdrew the wire, slid the needle under the skin at least halfway, and squeezed the tube from the bottom up.
30 mg of morphine tartrate entered the body. Within minutes, the world changed. And then you pin the empty tube to the wounded man’s collar. Needle through the fabric so the next person to reach him could see at a glance, “This soldier has already received morphine. Do not give more.
” That small ritual, the pin on the collar, is one of the most revealing details of the entire American system. Remember it because it tells you something that no German military planner in 1944 would have understood. The pin assumed that multiple people would reach the same wounded man. Not one rescuer, a sequence, a chain. The pin was not a medical procedure.
It was a signal from one link in that chain to the next. Now, think back to what that German doctor observed at Anzio. Nine Americans with shattered bones and open abdomen, none of them screaming. The set explains the silence. A half grain of morphine injected in the field within minutes of being hit could take the sharp edge off a compound fracture could turn a scream into a clenched jaw could make a man with a hole in his side sit up and ask for water instead of convulsing on a stretcher.
But here is what the set does not explain. A tube of morphine sitting in a bag does nothing. Someone has to bring it forward. Someone has to find the wounded man. Reach him. Kneel beside him in the open. Judge the wound. Break the seal. Slide the needle under skin. Squeeze the tube. Pin it to the collar.
And move to the next soldier down. Not in a hospital, not behind a wall. On the ground under the same fire that put the first man down. In the German army, the first person authorized to administer morphine was the battalion medical officer, an arst stationed at the troopen verbond plots, typically several hundred meters behind the front line, often farther.
A wounded German soldier lying in a ditch had to be found by a sanitator, dragged or carried to a collection point, and then transported rearward to the aid station before any painkiller touched his bloodstream. In winter, on broken terrain, under artillery, that journey could take an hour, sometimes two. Sometimes the man bled out before the sanitator reached him at all.
In the American army, the morphine did not wait at the battalion aid station. The morphine came forward. It traveled in a canvas bag on the hip of a man who was already there, already embedded inside the platoon, already 20 or 30 yard from the point of impact. And that man carried not one curette but 10. He was called a company aidman.
The infantry just called him Doc. Every rifle company in the United States Army had three of them, one per platoon. A battalion of 400 men had roughly 30. They carried no rifle. They wore a Red Cross brasard on the left arm and a Red Cross on the helmet. And they were expected to do something that no training manual could truly prepare a man for.
to hear the cry, to stand up, and to run toward the gunfire while every other living creature on that ground was trying to get away from it. What that job looked like in practice, what it cost the men who did it, and what it gave every American soldier who ever went down with an earshot, begins on a beach in France, 10 months after the surgeons at Venifro first noticed that their patients were arriving with too much morphine already in their veins.
June 6th, 1944, Omaha Beach, Normandy. The ramp of a Higgins boat dropped into chestde water off the coast of France, and technical sergeant Ray Lambert stepped into the sea for the third time in this war. Lambert was 23 from Alabama. He had been a company aidman with the 16th Infantry Regiment, First Infantry Division, since before North Africa.
He had won a silver star in Tunisia for driving a jeep under direct fire to reach wounded men. He had waited ashore at Sicily. By the morning of the 6th of June, he had been treating casualties in combat for a year and a half. He carried no rifle. He carried a canvas medical bag with bandages, sulfa powder, tourniquets, and 10 morphine ceretses, and he had 31 men on his landing craft.
Seven of them would be alive by nightfall. The machine gun fire began before the ramp hit the water. Men went down in the surf carrying 80 lb of gear and never came up. Lambert pushed forward, grabbing soldiers by their pack straps, rolling them face up, checking for breath. The water around him turned pink inside the first minute.
He reached the sand and began working, dragging wounded men behind the nearest steel obstacle, cutting away fabric, pouring sulfa powder into holes that minutes ago had been skin, squeezing ceretses into arms and thighs, and pinning the empty tubes to collars while mortar rounds walked across the beach.
Then something tore into his own leg. The wound open to the bone. Lambert looked at it, wrapped a tourniquet above the knee, pulled a serette from his bag, pushed the needle into his own thigh, squeezed, pinned the tube to his own collar, and went back to work. Think about that sequence for a moment.
A man with a wound deep enough to see bone in the middle of the largest amphibious invasion in history with machine guns firing from the bluff above him calmly applied his own tourniquet, injected himself with morphine, marked the dose on his collar, and returned to treating other soldiers. Not because he was superhuman, because his training had made the sequence automatic.
Tourniquet, set, pin, move. He kept going. He pulled men out of the rising tide. He bandaged a soldier whose arm was nearly severed. And then another round hit him, a blast that drove fragments into his back. And he tried to hand his medical bag to a second aidman who had crawled over to help.
He was shouting instructions over the noise of the shelling. He could not hear his own voice. And in the middle of that sentence, a bullet went through the other medic’s head. Lambert kept moving. He went back into the water. He dragged out another man, then another, and then a landing craft barreled in through the surf, dropped its ramp, and the steel slab came down directly onto Lambert’s lower back, crushing the fourth and fifth vertebrae and driving him to the bottom. Somehow, the boat backed off.
Somehow, Lambert surfaced. Somehow, with a broken spine and a leg split to the bone and shrapnel in his back, he pulled the other soldier to the beach. Then, his body stopped answering. He was loaded onto an evacuation craft. And here is a detail that belongs in this story because it tells you something about the scale of what happened that morning.
On that same craft, a Navy doctor checked Lambert’s dog tags and said, “We have another Lambert here.” Ray’s brother, Ule, also in the 16th Infantry, also wounded in Normandy, was lying on a stretcher a few feet away. They were evacuated on the same boat, transported in the same ambulance, delivered to the same field hospital in England, and wheeled into the same operating room.
When Rey woke up in the recovery ward, his brother was in the bed beside him. The first thing Ule said was, “What are you doing here? What’s mother going to say about this?” Both survived. Now, hold that story in your mind and consider the arithmetic. Lambert was one of three aidmen in his rifle company. His regiment, the 16th Infantry, lost seven medics killed and 24 wounded on the 6th of June alone.
Across the whole of Omaha Beach that morning, medics were doing what Lambert did, running into fire with no weapon, kneeling over broken men, squeezing cigarettes, pinning tubes, dragging bodies through surf, absorbing bullets meant for someone else. On a beach a few miles to the west, a Ponobskot Indian named Charles Sheay, also an aidman with the 16th Infantry, held a fellow medic named Edward Morzich in his arms.
Private Morzich was dying from a stomach wound. Sheay bandaged him and gave him morphine, knowing it would not save him. Then he moved to the next man. This is what the American system looked like at the point of contact. Not a hospital, not a doctor. A 23-year-old from Alabama with a canvas bag and 10 tin tubes, standing between a wounded soldier and the worst pain of his life, doing it again and again and again until his own body broke.
And here is what should unsettle you. On that same 6th of June, across that same beach, German soldiers were also being hit. German defenders in the bunkers above Omaha were taking naval gunfire, aerial bombing, rifle rounds from below. They were being wounded in the same ways. Shrapnel, bullets, blast concussion, burns. And when a German soldier went down inside his position, what reached him was not a medic with a bag of ceretses.
What reached him was a soneta carrying a single furbon pexction, a small cloth bandage, and nothing else. No morphine, no sulfa, no plasma, a bandage and a prayer that the battalion doctor was still alive somewhere to the rear. What that difference looked like from inside a German bunker and what it reveals about two armies that were fighting the same war with entirely different ideas about what a soldier’s life was worth is the darkest part of this story.
On the morning of the 6th of June, inside a concrete imp placement above Omaha Beach, a German machine gunner was firing through an embraaser slit when a naval shell detonated against the outer wall of his position. The blast did not penetrate the bunker, but it sent a shock wave through the concrete that shattered the gunner’s left forearm and drove fragments of his own weapon into his chest. He fell behind his gun.
A zanita, the German equivalent of a medic, reached him within minutes. The zanyeta opened a viband pexion, the individual bandage packet that every German soldier carried. He wrapped the arm. He checked the chest wound, decided it was not immediately fatal, and tied a second bandage across the torso.
Then he looked at the wounded man, and had nothing else to offer. No morphine, no sulfa powder, no plasma, no ceret, no injection of any kind. The zanita was trained to bandage, splint, and carry. He was not trained to administer drugs. He was not authorized to administer drugs. The first person in the German chain of evacuation who could give this man anything for the pain was a medical officer at the Tupin Vaband plat, the battalion aid station somewhere behind the bluffs.
If it was still standing, if the officer was still alive, if the route between here and there was not already cut by American fire. The wounded German lay on the concrete floor of a bunker, fully conscious with a shattered arm and steel in his chest and waited. That was the system. Not because Germany lacked morphine, not because German medicine was primitive, but because the German military had made a decision, a decision so deeply embedded in the structure of the vermach that no one in it thought to question it.
That pain relief was a medical act. and medical acts belong to doctors and doctors belonged at aid stations, not in foxholes. The American army had made the opposite decision and the distance between those two choices was the distance between silence and screaming. Now, if this were only about morphine, about one drug in one tube, the story would end here.
But the morphine curette was the visible edge of something much larger. To understand what the Germans were actually seeing when they looked at those quiet American wounded, to understand why it baffled them, you need to see what the German medical system looked like from the inside. In May of 1945, days after the German surrender in Italy, the Fifth Army surgeon sent a team of American medical officers to inspect the captured German military hospitals, surgical stations, and aid posts across the Italian peninsula.
These were experienced men, colonels and lieutenant colonels who had spent 2 years operating on casualties in North Africa, Sicily, Anzio, and the drive up the boot. They knew what good battlefield medicine looked like. They had built it. And what they found in the German installations left several of them unable to finish their inspections.
At one hoped Faban Platz, a forward surgical station roughly equivalent to an American clearing company, the observers watched a German surgeon perform wound surgery on a series of casualties. The surgeon incized the skin, cut the fascia, removed the most obvious debris, trimmed the edges of dead tissue, and moved to the next patient. He did not excise the wound.
He did not clean the deeper layers. He drained the wound and closed it, leaving devitalized tissue inside. Then he set his instruments on the tabletop and walked to the next stretcher without washing his hands. The American observer left the room without shaking the surgeon’s hand. In a conversation afterward, a German medical officer explained what the Americans were seeing.
In the German army, he said, it was assumed automatically that every penetrating combat wound would become infected. PUS was anticipated. PUS was not a complication. It was the expected outcome. The goal was not to prevent infection. The goal was to manage it after it arrived. One German surgeon reported that in 5 years of performing war surgery, he had carried out only four or five thorough wound excisions of the kind that every American surgeon performed as routine. Four or five.
in five years. The American medical team compiled their findings into an official report. The historian Anthony Beaver, drawing on records from the same period, described what they found in blunter terms. “A German failed Lzerette,” he wrote, was little more than an amputation line. “American doctors were horrified by the German army’s readiness to cut off a limb without a moment’s deliberation.
” And here is a detail that brings this down from systems to a single human being. At the Bushnell General Military Hospital in Utah, an American facility that treated both Allied and Axis wounded, a German prisoner of war was brought in with a badly infected arm wound. The American doctors treated it with a drug the prisoner had never seen, a yellowish powder derived from a mold administered by injection.
Within days, the infection retreated. The arm was saved. The German soldier told his doctors that in the German army, a surgeon would have amputated immediately. He had never heard of the drug. He asked what it was called. They told him penicellin. The nation that had produced Bayer, that had built EJ Farbin into the largest chemical conglomerate on Earth, that had invented aspirin and synthesized heroin and manufactured pervatin by the millions of tablets, could not produce penicellin for its own soldiers.
They tried. EJ Farbin tried. They even attempted to steal Alexander Fleming’s original mold from his laboratory in London. But mass production of penicellin required a kind of coordination between government, industry, and medical research that Germany in 1944 simply could not achieve. The United States could.
And what that coordination looked like, the scale of the machine that stood behind every company aidman with his canvas bag and his 10 ceretses, is what finally answers the question in the title of this story. Because the Germans could not explain what they were seeing for a reason that had nothing to do with one drug or one medic or one hospital.
They could not explain it because they were looking at the visible tip of an industrial system that did not exist anywhere else on Earth. Here is what stood behind the aidman with the canvas bag. When Ray Lambert pinned a morphine ceret to a wounded soldier’s collar on Omaha Beach, he had already done two other things that the German medical system could not match.
He had torn open a packet of sulfanylamide powder and poured it directly into the open wound. A white crystallin dust that killed bacteria on contact. And he had tied a muslin bandage prepacked and sterile around the injury tight enough to slow the bleeding but loose enough to keep circulation alive. three acts, set, sulfa, bandage.
Together, they took less than 90 seconds. And in those 90 seconds, the wounded soldiers odds of surviving shifted from the mathematics of the Civil War to the mathematics of the 20th century. But the aidman’s work was only the first 60 seconds of a chain that stretched 4,000 m from the wet sand of Normandy to a hospital bed in Virginia.
And every link in that chain existed because someone in the United States had built it, supplied it, and shipped it across an ocean before the first bullet was fired. Take one link. Blood plasma. A wounded soldier who had lost blood was dying of shock. His blood pressure was dropping. His organs were shutting down. Morphine could quiet his pain, but it could not replace what was leaking out of him.
He needed volume. fluid in his veins, something to keep his heart pumping until a surgeon could close the holes. On any battlefield before 1941, that man was dead. On Omaha Beach, a medic could save him. Inside the medical supply crates that washed ashore with the infantry were packages containing two tin cans.
One held a bottle of dried plasma, a pale yellow powder, light as dust. The other held a bottle of sterile distilled water and a length of rubber tubing with a needle. The medic mixed the water into the plasma, shook the bottle until the powder dissolved, hung the bottle from whatever was vertical. A rifle jammed bayonet first into the sand, the frame of a wrecked vehicle, a piece of driftwood, and slid the needle into the soldier’s vein.
Within minutes, the blood pressure began to climb. The organs got oxygen. The man lived long enough for a surgeon to reach him. That bottle of dried plasma on the beach at Normandy had begun its life as a pint of blood in the arm of a stranger in Omaha, Nebraska or Duth, Minnesota or Birmingham, Alabama.
A stranger who had walked into a Red Cross donation center or climbed aboard one of the mobile collection trucks that Americans had taken to calling blood mobiles and given blood for a man he would never meet. The scale of what happened next is difficult to hold in your mind. So, let me give you one number and then show you what it means.
By the end of the war, the American Red Cross had collected more than 13 million pints of blood. 33 processing centers across the country converted that blood into dried plasma, a form that could survive heat, travel without refrigeration, and sit in a crate on a beach head for weeks without losing potency. More than 10 million units of dried plasma were produced in the United States and shipped overseas.
10 million. Each unit was a bottle. Each bottle was a life that could be pulled back from the edge. And each one had started as a voluntary donation from a civilian who would never hear a shot fired. The man who made this possible was a surgeon named Charles Drew. He was the first African-Amean to earn a doctor of science degree.
He had developed the technique for processing and preserving plasma on an industrial scale. He designed the mobile blood collection stations. He directed the Red Cross pilot program that proved the system could work. And then in one of the wars quieter cruelties, the army he was supplying with the means to save lives segregated the blood he collected by the race of the donor.
Drew pointed out publicly that there was no scientific basis for the policy. He was quietly removed from the program. The plasma kept flowing. By June of 1944, the month of the Normandy invasion, Red Cross centers were collecting more than 500,000 units of blood in a single month. Factories were freeze drying plasma around the clock.
Ships were carrying crded bottles across the Atlantic in convoys. And on the morning of the 6th of June, when medics crawled across Omaha Beach, hanging plasma bottles from rifle stocks, they were the final inch of a supply line that ran from the arm of a housewife in Kansas City to the vein of a 19-year-old private with a hole in his lung.
Germany had nothing remotely like this. The German medical service used blood substitutes, a synthetic colloid called paristin, a physiological saline solution administered at the helped verban plots, the forward surgical station miles behind the front. Direct blood transfusions were performed occasionally, but always doctor to patient, never from a stored supply.
There was no national blood collection program, no dried plasma, no bottled reserves sitting in crates at the front. A German soldier bleeding out in a ditch was waiting for a doctor with a syringe and a donor if one could be found. And that doctor was miles away. Now go back to the number I asked you to remember in part one.
Three out of four of Beecher’s wounded soldiers at Anzio said they did not need morphine. Beecher believed this was about psychology, the meaning of the wound. And he was partly right. But there is another explanation he did not consider because it was invisible to him. By the time those men reached Beecher’s table, they had already been found by an aidman.
They had already received morphine, sulfa, and a bandage within minutes of being hit. Many had already received plasma. Their pain had been blunted. Their infections had been slowed. Their blood pressure had been stabilized. They arrived at the hospital not as raw casualties, but as men who had already been treated by the most forward deployed medical system in the history of warfare.
They did not need morphine at the hospital because the morphine had already reached them in the field. But even plasma and sulfa and ceretses do not fully explain what the Germans were seeing. Because behind the supply chain, there was something else. a decision made years before the first shot about what kind of army America was going to build.
And that decision had consequences that went far beyond medicine. To understand that decision, you need to see what each army chose to put into the hands of its soldiers before the war began. Not what they gave them to fight with, what they gave them to survive with. Because that choice tells you everything. In the spring of 1939, 6 months before Germany invaded Poland, the Timler Pharmaceutical Company in Berlin began shipping a new product to the Vermacht in bulk.
It came in small tubes of tablets stamped with the label pervatin. The active ingredient was methamphetamine, crystal meth. Between April and December of 1939, Timler delivered 29 million pervatin tablets to the German military. Millions more followed during the Blitzkrieg through France in 1940. The tablets were distributed to tank crews, pilots, infantry, submariners.
They suppressed fatigue, sharpened aggression, and allowed soldiers to fight for days without sleep. Vamach medical officers called them a tool for extending human performance under extreme stress. 29 million tablets of methamphetamine. That was the drug Germany chose to mass-produce for its soldiers.
Now, hold that number and consider what the United States was doing in the same period. In the spring of 1943, a year before D-Day, the War Production Board in Washington sat down with representatives from more than 20 American pharmaceutical companies and laid out a plan. The objective was not to make soldiers fight longer. The objective was to keep wounded soldiers alive. The product was penicellin.
The problem was scale. Alexander Fleming had discovered the mold in London in 1928. Howard Flory and Erns Chain at Oxford had proven it could kill bacteria in living patients. But producing enough penicellin to treat a single man took weeks of growing mold in shallow trays, a process so slow that by early 1943, the entire British and American supply could treat roughly 10 patients.
The War Production Board identified four steps. Find a strain of the mold that produced more penicellin. find a way to grow it in industrial quantities, find an efficient method of extraction, and package it in consistent deployable doses. What happened next was something the German system for all its brilliance in chemistry, for all the power of IG Farbin, could not replicate.
21 American companies agreed to cooperate, not compete, cooperate. Fizer, Merc, Squib, Abbott, Lily, firms that in peace time fought each other for market share, opened their laboratories to one another. A researcher at the Northern Regional Research Laboratory in Peoria, Illinois, found a cantaloupe in the facilities cafeteria with a particularly potent strain of penicyium growing on its rind.
A chemical engineer named Margaret Hutchinson Russo working for Fizer designed a deep tank fermentation system that could grow the mold in 20,000galon vats instead of shallow trays. By the morning of the 6th of June 1944, the United States had produced approximately 2.3 million doses of penicellin, enough for every Allied soldier who would be wounded on the beaches of Normandy.
Here is what that meant on the ground. Before penicellin, a soldier with a deep shrapna wound faced a simple equation. The wound would become infected. The infection would spread. If it reached the bone, the limb was lost. If it became gas gang green, a condition where bacteria consumed living tissue and released poison into the bloodstream.
The soldier was dead within days unless a surgeon amputated fast enough to outrun the rot. Among Allied troops who received penicellin in the field, gang green occurred at a rate of 1.5 cases per thousand wounded. Among German prisoners captured later in the war who received only sulfonomide, the older weaker antibiotic, the gang green rate was 20 to 30 per thousand, more than 15 times higher.
A surgeon in the 56th Evacuation Hospital, writing in his diary after the first large-scale use of penicellin in the European theater, put it in five words. We snatched them from the grave. Now, step back far enough to see both pictures at once. Germany gave its soldiers methamphetamine to make them fight longer.
America gave its soldiers morphine to stop the pain, sulfa to stop the infection, plasma to stop the bleeding, and penicellin to stop the gang green. Germany’s drug kept a man in the fight. America’s drugs kept a man alive. This was not a failure of German science. German chemists were among the finest in the world.
Germany had synthesized aspirin, heroin, methadone, and methamphetamine. Germany had Fritz Hobo who had fixed nitrogen from the air. Germany had IG Farbin, the largest chemical enterprise on the planet with more industrial capacity than most nations. But IG Farbin could not produce penicellin because penicellin required something IG farbin did not have.
It required 21 competing companies to stop competing. It required a government that could coordinate industry, academia, and the military toward a single humanitarian objective. It required a nation that believed the purpose of its industrial power was not just to build weapons, but to save the men who carried them.
Germany used its chemical genius to build nerve gas. America used its chemical genius to build penicellin. And that distinction, that single fork in the road, is the answer to the question in the title of this story. The Germans could not explain how wounded Americans felt no pain because they were not looking at a drug. They were not looking at a medic.
They were not even looking at a supply chain. They were looking at the output of a civilization that had made a decision their own civilization had not. The decision was this. Every soldier is coming home. Not every soldier will survive. But every soldier will be treated as if he can. Every wound will be met with morphine, sulfa, plasma, and penicellin.
Every broken body will enter a chain of evacuation designed to move it rearward faster than death can move forward. Every man matters enough to spend the resources. The German army never made that decision, and the men who paid for it were the men on the ground. On the morning of the 6th of June 1944, about 6 milesi inland from Utah Beach, two American medics landed by parachute in a Normandy pasture and made their way to a 12th century stone church in the village of Anggoville Oplane.
Their names were Robert Wright and Kenneth Moore. They were privates in the 501st Parachute Infantry Regiment, 101st Airborne Division. They carried no weapons. They carried medical bags and within an hour of landing the wounded started coming. Wright and Moore cleared the pews, laid stretchers and blankets across the stone floor and turned the Church of Saints Cosmos and Damian into a forward aid station.
They set one rule. Anyone who came inside, American or German, left his weapon at the door. Through the morning and into the afternoon, the village changed hands. American paratroopers pushed in. Germans pushed back. The front line rolled through Angleville Oplan like a tide. And through all of it, Wright and Moore stayed inside the church, treating whoever was carried through the door.
American soldiers arrived with bullet wounds. They got morphine, sulfa, bandages. German soldiers arrived with shrapnel injuries. They got the same morphine, the same sulfa, the same bandages. Behind the altar, Wright and Moore placed the men they knew would not survive, and they gave those men morphine, too.
Not to save them, to let them leave quietly. Around midday, the door burst open. A German soldier stood in the entrance holding an MG42 machine gun. He had been fighting all morning. He scanned the room. the rows of broken men on the floor, the two unarmed Americans kneeling between them, the German wounded lying beside American wounded receiving identical treatment.
He looked at the medics. The medics looked at him. He lowered the gun. He made the sign of the cross and he walked back out into the war. Later that afternoon, a German officer arrived with two enlisted men. Moore told him the same thing he told everyone. Leave the weapons outside or do not come in. The officer protested. Moore did not move.
The officer left his pistol at the door. Here is what I want you to see in that church because it answers the question this story has been building toward for the last 40 minutes. A wounded German falshroom, a paratrooper, the best the Vermacht had, lay on a stone floor in a French church and received from the hands of an American private the same half grain morphine curette that every wounded American received, the same sulfa powder, the same sterile bandage, the same human attention.
That German paratrooper’s own army had not given him any of those things. His own sanitator carried a cloth bandage and nothing else. His own system required him to reach a doctor before the pain could stop. His own fa loterette, if he ever got to one, would likely have cut off a shattered limb rather than try to save it.
His own nation, the nation that had isolated morphine that had built Bayer that had synthesized every painkiller on the pharmacy shelf, had sent him into combat with a bandage and methamphetamine. And now lying wounded on the floor of an enemy’s aid station, he was receiving better medical care than his own army had ever been designed to provide. That is the answer.
The Germans could not explain how wounded Americans felt no pain because the explanation required understanding a system built on a principle that the German military did not share. The principle was not medical. It was moral. It was the decision that a wounded soldier is not a spent cartridge. He is a man with a family and a life to return to.
And the full weight of the nation’s science, industry, and logistics should be pointed at keeping him alive. Morphine was the instrument. The medic was the delivery system. Plasma was the bridge. Sulfa was the shield. Penicellin was the miracle. But beneath all of it was an idea. And the idea was that the pain of one private lying in one ditch on one beach mattered enough to mobilize 13 million blood donations and 21 pharmaceutical companies and 30 medics per battalion and 10 curettes per bag.
Germany did not fail because it lacked chemistry. Germany failed because it never asked the question that would have led to the curret, the aidman, the plasma bottle and the penicellin vial. The question was not how do we make soldiers fight harder. The question was what happens to a man in the first five minutes after he is hit and the German army never considered that question worth answering at the level of the individual soldier.
The result was arithmetic. The American army’s mortality rate for battle casualties dropped from 8.1% in the first world war to 3% in the second. By June of 1944, the overall surgical survival rate in the European theater reached 80%. Even for abdominal wounds with damage to the internal organs, the most lethal category of battlefield injury, the survival rate was 68%.
In the German medical system, a soldier with the same abdominal wound entered a chain where the surgeon did not wash his hands between patients, where wound excision was a rarity, where pus was expected, where amputation was the default, and where penicellin did not exist. The gap between 3% mortality and whatever the German figure was, a number the Vermach did not survive long enough to calculate honestly, is the gap between two ideas about what a nation owes the men it sends to die.
And the men who lived inside that gap, the men who survived because the system reached them and the men who did not survive because no system came are the reason this story is not really about medicine at all. It is about what happened to them afterward and that is where it ends. After the war, Henry Beecher went home to Harvard.
He published his paper on pain in wounded soldiers in January of 1946. The medical world read it and did not fully understand what he was telling them. Not then. It took years. Beecher kept working. He studied the placebo effect with a rigor that no one before him had attempted. He showed that a saline injection given with conviction could replicate 90% of morphine’s pain relief in wounded soldiers.
He proved that the mind is not a passenger in the body. It is the driver. And then he did something else. He went to Bukinva. Beecher was among the first American medical professionals to investigate the surgical experiments that Nazi doctors had performed on concentration camp prisoners. He examined the records. He interviewed the survivors.
And what he found changed his career a second time. He became one of the earliest and most forceful advocates for informed consent in medical research. The principle that no experiment may be performed on a human being without that person’s knowledge and agreement. His 1966 paper on ethics and human experimentation is considered one of the founding documents of modern medical ethics.
The man who had knelt in the mud at Anzio, counting soldiers who did not need morphine, spent the rest of his life making sure that the science born from that mud would never be used the way Germany had used its science. He died in 1976 at the age of 72 in Boston. Ray Lambert went back to Alabama. He married.
He raised a family. For decades, he did not speak about what happened on the beach. The memories lived in his body. The crushed vertebrae, the scar down his leg, the shrapnel the surgeons never removed. His brother Ule survived, too. They both carried Omaha Beach for the rest of their lives without discussing it, the way men of that generation carried things.
Then, in his 90s, Lambert began to talk. He gave interviews. He wrote a memoir. And in 2019, at the age of 98, he went back to Omaha Beach. He stood on the sand where he had pinned ceetses to collars and dragged men from the surf and injected his own leg with morphine and kept going until a steel ramp broke his spine.
He stood there and he looked at the water and he said what he had never been able to say as a young man, that he had been afraid the entire time and that the training was the only thing that kept him moving. Charles Shea, the Ponobskot medic, who had held Private Morose in his arms and given him morphine, knowing it was the last kindness the man would receive.
Sheay left the army after Korea and eventually moved to France. He settled near Normandy. He spent his final years within a few miles of the beach where it all began. He died in December of 2025 at 101. The people of Normandy buried him as one of their own. Robert Wright and Kenneth Moore, the two privates who turned a stone church into a hospital and told armed men to leave their weapons at the door, both survived D-Day, the hedge, and the battle of the bulge.
The church at Anggoville Oplan still stands. It has stained glass windows now installed by the village honoring the two American medics who treated anyone who came through the door. If you visit today, you can still see the stains in the wood of the pews. 82 years later, the blood has not come out. Charles Drew, the surgeon who made the plasma program possible, died on the 1st of April, 1950 in a car accident in North Carolina. He was 45 years old.
The blood banking system he built outlived him by generations. It is still operating. Every pint of blood donated in the United States today moves through infrastructure that Drew designed. and the set, the collapsible tin tube that started this story. You can still find them in estate sales, in attics, in the drawers of men who carried them home and never threw them away.
They sit in museum cases now behind glass, next to helmets and dog tags and folded flags. Most of them are empty. The morphine is long gone. What remains is the tube itself. small, light, unremarkable, the kind of object you could hold in your palm and never guess that it once stood between a man and the worst moment of his life.
The Germans could not explain how wounded Americans felt no pain because they were looking at the wrong thing. They were looking at the silence and searching for a cause. But the silence was not caused by any single object or any single drug. It was the sound of a system. A system that began with a chemist in Brooklyn and a blood mobile in Kansas City and a cantaloupe in Peoria and 21 companies that agreed to stop competing and 13 million pints of blood from people who would never know whose life they saved.
Arriving at the side of a 19-year-old private before his pain had time to peak. The answer was never morphine. The answer was that someone came. Thank you for staying with this story for the past hour. If it meant something to you, the best thing you can do is hit the like button. It is the single biggest factor in helping a video like this reach people who would never find it otherwise.
If you are not yet subscribed, I would be honored if you joined this channel and turned on the bell so you never miss one of these histories. I would love to know where you are watching from today. And if someone in your family served in the Second World War, a father, a grandfather, a great uncle, anyone, I hope you will tell us about them in the comments.
These stories survive because people like you keep passing them forward. Thank you.